


Most patients with human monkeypox (HMPX) have cutaneous lesions. In the 2022 outbreak of HMPX across non-endemic countries, cutaneous lesions have been different than previously described.1,2 In this outbreak, primary lesions often occur at anogenital and oral sites, suggesting direct inoculation, similar to patterns observed with syphilis.3 Primary lesions may occur before, with or without the onset of systemic symptoms. Although secondary lesions continue to present in a disseminated fashion, developmental pleomorphism (the phenomenon of lesions at different stages of development at the same anatomic site), is seen more commonly than previous outbreaks in which lesions were classically monomorphic.4 Furthermore, new lesions can continue to emerge for several days.4,5 The lesions may resemble those caused by other infections including syphilis, herpes simplex virus, molluscum contagiosum or folliculitis.5
We present clinical images to show the breadth of cutaneous and mucocutaneous lesions that presented in 8 patients with HMPX (confirmed by real-time polymerase chain reaction) who were cared for in Toronto, Canada, from May to July 2022. None of these patients were notably immunocompromised by a condition (including uncontrolled HIV) or immunosuppressing medication, which may modify disease severity. Patients with well-controlled HIV are indicated accordingly in the captions. We include images of active primary lesions at common locations (Figure 1, Figure 2, Figure 3 and Figure 4) and of lesions showing developmental pleomorphism (Figure 5 and Figure 6). We also include images of active secondary lesions by stage of development, including macules, papules, pustules, umbilicated pustules and ulcers that then scab over and heal (Figure 7, Figure 8, Figure 9, Figure 10 and Figure 11). We provide images of lesions on the palms and soles (Figure 6 and Figure 9). In several cases, patients initially received diagnoses of, and were treated for, probable syphilis or herpes simplex virUs before a differential diagnosis of HMPX was considered.

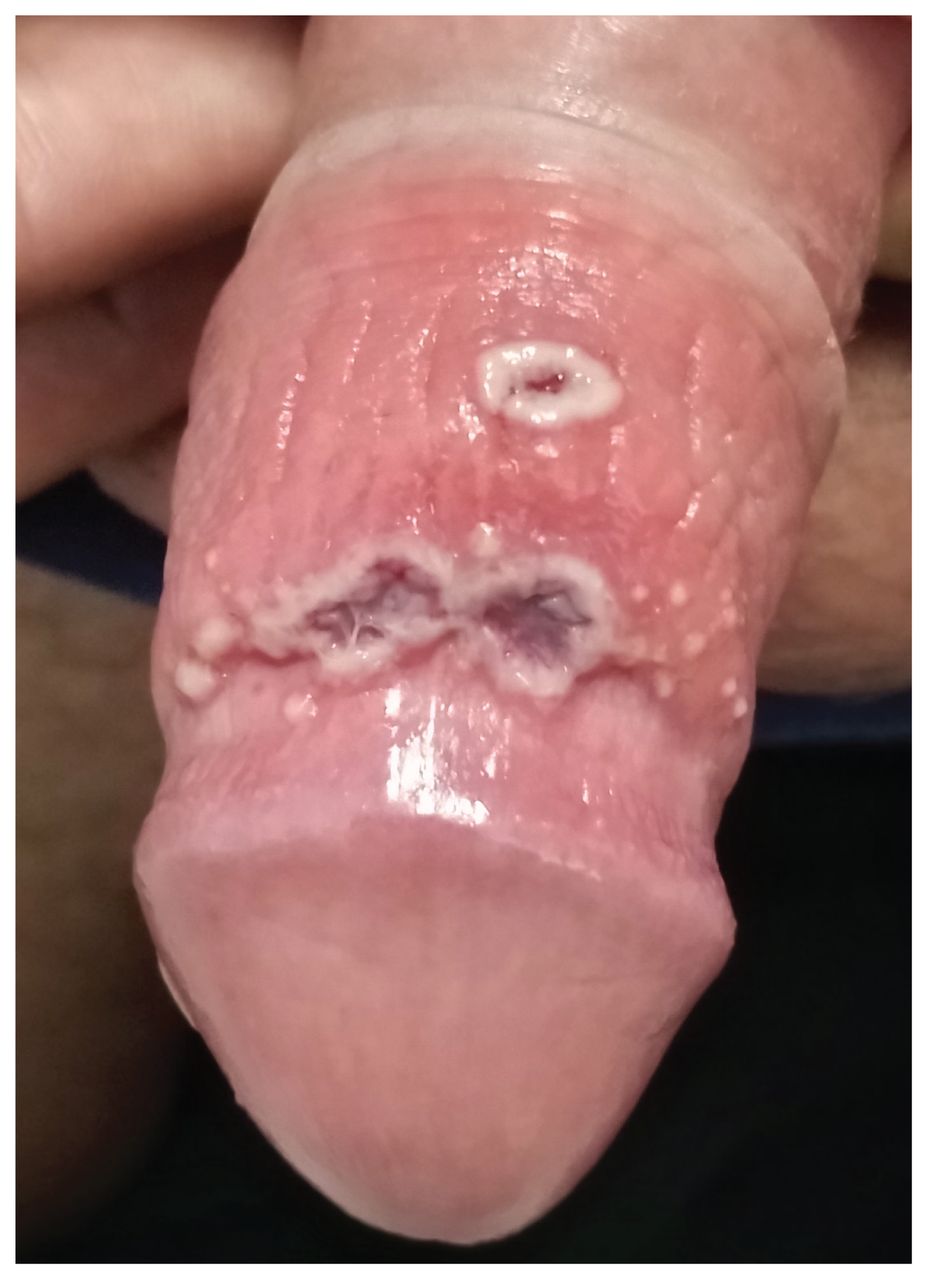
Primary penile lesions in a 26-year-old cisgender man with human monkeypox. (A) Numerous erythmatous, tender papules (pinpoint to 1 mm in diameter) scattered across the glans and distal penile shaft with the foreskin retracted, on lesion day 2. These were part of the primary crop of lesions that developed on illness day 1 and were not associated with systemic symptoms. Over 4 days, these papules progressed to pustules and umbilicated lesions. (B) Pustules from the same patient on lesion day 5.
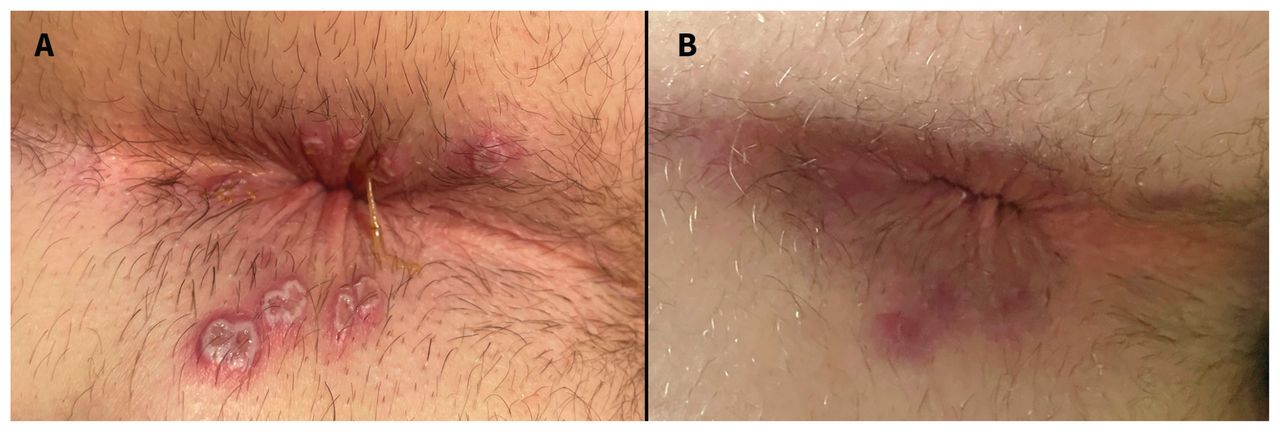
Primary perianal lesions in a 34-year-old cisgender man with human monkeypox. (A) Numerous exquisitely tender ulcers (2–10 mm in diameter) in the perianal region, on lesion day 6. Each ulcer had a moist, tan base; pearly white edges that were heaped up or rolled; and a peripheral rim of poorly demarcated, dark erythema. These lesions, part of the primary crop of lesions, developed on illness day 2. They were associated with substantial proctitis and bilateral tender inguinal lymphadenopathy. Oral opiates were required to manage the pain. (B) These lesions resolved at lesion day 17, after crusts formed and then desquamated, revealing re-epithelialized, healed skin with a diameter of hyperpigmentation smaller than the pustular stage of each lesion.

Primary perioral lesion in a 41-year-old cisgender man with human monkeypox and well-controlled HIV, on lesion day 7. Located on the right upper lip, the 12 mm ulcer with peripheral erythema was nonpruritic and nontender. This ulcer was part of the initial crop of cutaneous lesions and predated the onset of systemic symptoms. It was associated with new, tender, right cervical lymphadenopathy on a background of pre-existing bilateral cervical lymphadenopathy in the context of known HIV. On a follow-up visit on lesion day 21, this lesion had dried, crusted and desquamated, revealing healed skin.

Primary tongue lesion in a 56-year-old cisgender man with human monkeypox and well-controlled HIV, on lesion day 5. Located on the right tip of the tongue, the 5 mm ulcer was tender, with overlying purulence and surrounding edema. On the left posterior aspect of the dorsal tongue was a focal swelling surrounding another ulcer that is not visualized here. These ulcers, part of a primary crop of lesions, were the patient’s initial clinical presentation and were associated with bilateral cervical lymphadenopathy, odynophagia and oropharyngeal dysphagia. The latter 2 symptoms prompted the start of oral tecovirimat on lesion day 7.

Developmental pleomorphism of lesions in a 25-year-old cisgender man with human monkeypox, on lesion day 9. Located on the penile shaft immediately beneath the glans, the pair of 10 mm, tender ulcers had grey-purple bases and pearly white rolled edges. They were associated with bilateral, tender, inguinal lymphadenopathy. These 2 ulcers were first recognized as 1 mm, nontender, pruritic pustules on illness day 1. On illness day 5, the patient developed fatigue, myalgias and bilateral groin pain, followed by rapid, painful enlargement and ulceration of both pustules on illness day 7. The third lesion, located proximal to the initial pair of ulcers, developed on illness day 3 and progressed in a similar fashion as the initial pair of lesions. In the 48 hours before this image was taken, numerous 1–2 mm tender pustules developed adjacent to the first 2 ulcers. These were associated with erythema and edema of the foreskin and the glans and shaft of the penis. This image shows pleomorphism, the simultaneous presence of different stages on a single anatomic area. This patient received valacyclovir for a presumed genital herpes simplex virus infection at a community sexual health clinic, which was stopped when the lesion tested negative for herpes simplex virus by polymerase chain reaction.

Secondary lesions on the sole and feet of a 56-year-old cisgender man with human monkeypox and well-controlled HIV, on lesion day 11. This image depicts developmental pleomorphism (i.e., multiple lesions at various stages of healing on the same anatomic area). Visible lesions included a macule (base of left third toe), papule (left dorsal midfoot), pustules (right medial ankle, left dorsal foot), crusted lesions (right sole) and healed lesions whose crusts had recently desquamated (right medial ankle and left lateral forefoot). These lesions, part of a secondary crop of lesions that developed over 9 days, were nontender and nonpruritic. At the time of this image capture, this patient was receiving tecovirimat.

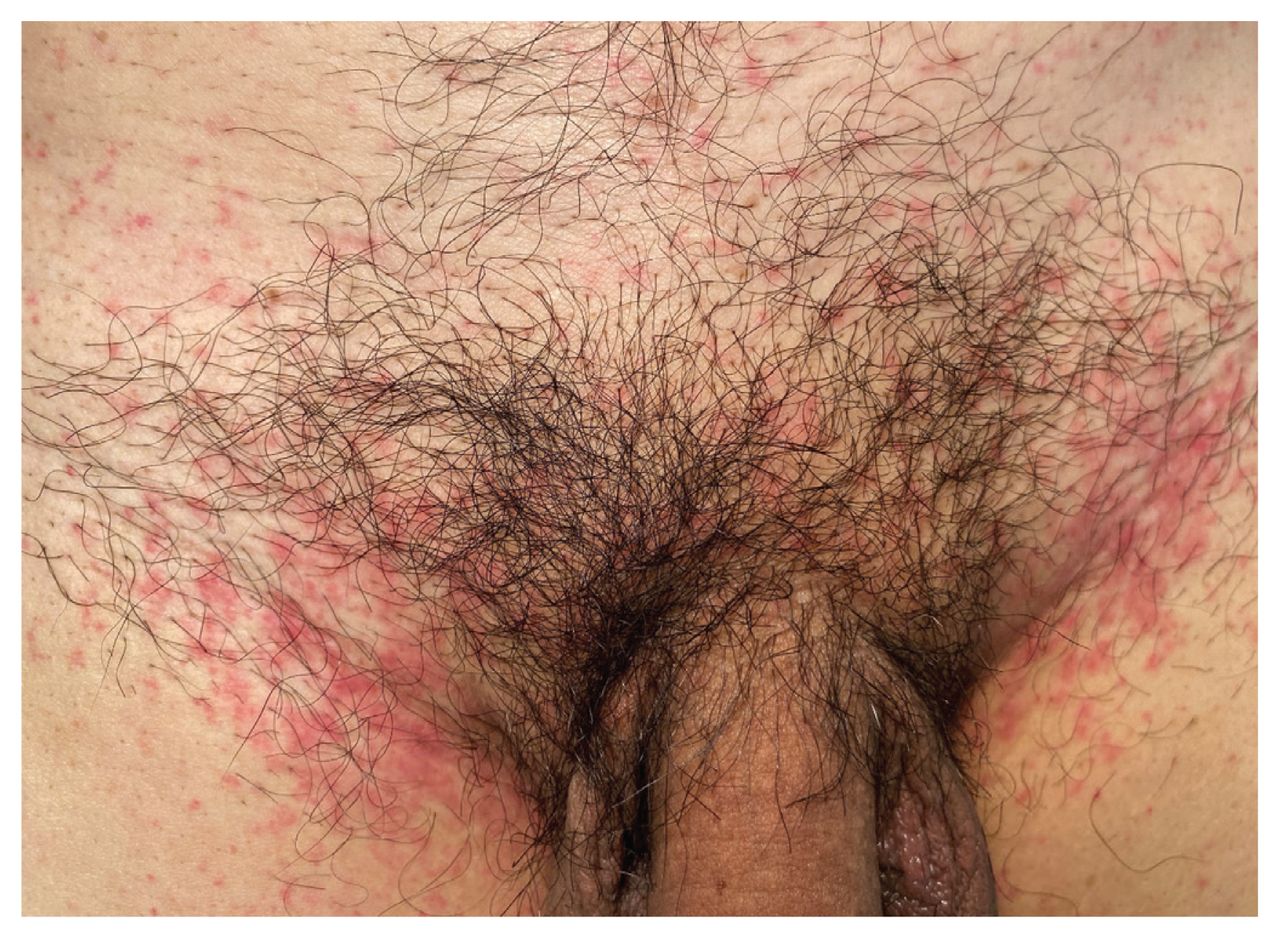
Secondary macules and papules in a 60-year-old cisgender man with human monkeypox and well-controlled HIV, on lesion day 1. Numerous 1–3 mm erythematous, mildly pruritic macules and papules were in the pubic region. These lesions, part of a secondary crop of lesions, developed on illness day 7, and were coalescing in the bilateral inguinal folds. Before the onset of this rash, the patient had developed a febrile prodrome (fever, chills, malaise and headache) on illness day 1, followed by bilateral tender inguinal lymphadenopathy on illness day 2 and vesiculopustular rash on the face and perianal area on illness day 5.
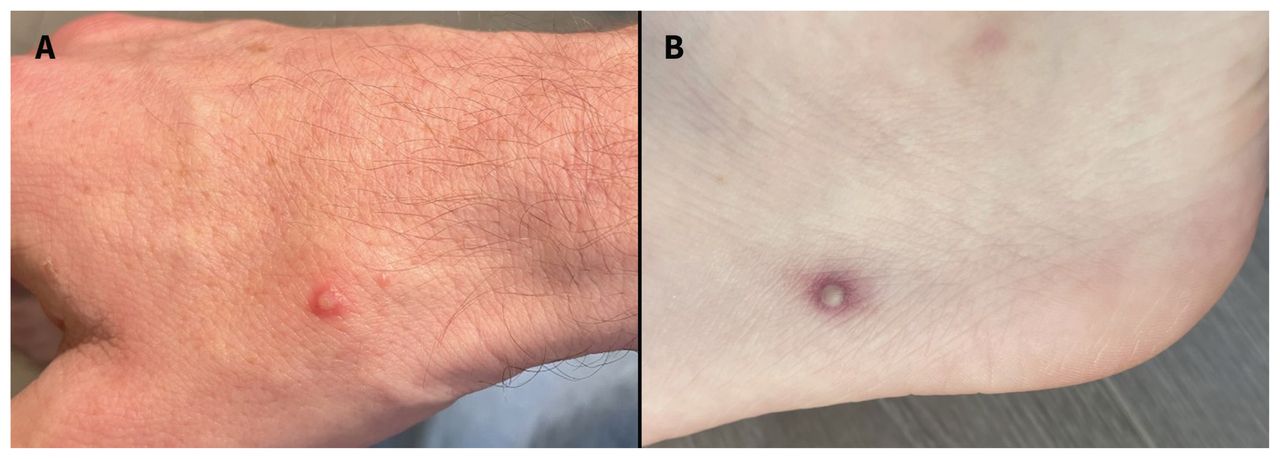
Secondary pustules in a 34-year-old cisgender man with human monkeypox. (A) On lesion day 2, a 2 mm pustule at the base of the right dorsal thumb was pruritic and nontender, with a small rim of well-demarcated erythema. This pustule, part of a secondary crop of lesions, had no associated regional lymphadenopathy when it developed on illness day 6. It ulcerated and crusted over by lesion days 4 and 6, respectively. (B) On lesion day 3, a 4 mm pustule with peripheral erythema on the patient’s left lateral heel was neither pruritic nor painful. This pustule, part of a secondary crop of lesions, developed on illness day 8 and was crusted by lesion day 9.

Secondary palmar pustules. (A) Four 1–3 mm pustules (arrows) on the left palm of a 56-year-old cisgender man with human monkeypox and well-controlled HIV, on lesion day 3. The pustules, part of a secondary crop of lesions, were surrounded by poorly demarcated erythema, developed on illness day 10 and were not associated with axillary lymphadenopathy. (B) A 3 mm, nonpruritic, tender pustule on the left palm of a 40-year-old man with human monkeypox and no immunocompromising conditions, on lesion day 3. The patient was taking emtricitabine–tenofovir disoproxil fumarate for HIV pre-exposure prophylaxis. Although this lesion was deep to the epidermis, a swab of its unroofed surface tested positive for monkeypox virus on polymerase chain reaction. This pustule, part of a secondary crop of cutaneous lesions, began on illness day 3, after the simultaneous onset of a febrile illness (fever, chills, myalgias, fatigue) and primary genital lesions on illness day 1.

Secondary umbilicated pustule on a 34-year-old cisgender man with human monkeypox, on lesion day 3. Located on the antecubital fossa, the 2 mm pustule had central umbilication and peripheral poorly demarcated erythema. This pustule, part of a secondary crop of lesions, developed on illness day 6, was pruritic until the ulcer stage and had no regional lymphadenopathy. The crust had fallen off by lesion day 16.

Temporal progression of facial lesions in a 50-year-old cisgender man with human monkeypox and well-controlled HIV. These 2 lesions, part of a secondary crop of lesions, developed on illness day 6 and were associated with ipsilateral submandibular lymphadenopathy. The preauricular lesion on the left was also associated with mandibular (V3) trigeminal neuralgia, which resolved as the lesion crusted. (A) On lesion day 4, the left (10 mm) and right (7 mm) ulcers were developing crusts, surrounded by light, poorly demarcated erythema. (B) On lesion day 7, the left lesion (14 mm) was nonpruritic, nontender and had an adherent dry crust. The right lesion (11 mm) was nonpruritic, nontender and healing, photographed 10 minutes after the crust fell off. (C) On lesion day 8, the lesions showed early re-epithelialization after the crusts fell off. (D) On lesion day 12, the fully healed lesions left hypertrophic pox scars.
Acknowledgements
The authors acknowledge Dr. Adrienne Chan for her substantial contributions to this publication. The authors also acknowledge patients who have allowed them to share their images and stories.
Footnotes
Competing interests: Darrell Tan reports research support from Abbvie, Gilead and Glaxo Smith Kline. Sharmistha Mishra is supported by a Tier 2 Canada Research Chair in mathematical modelling and program science. No other competing interests were declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

